Ian Ashdown, P. Eng. FIES, Senior Scientist, SunTracker Technologies Ltd.
Published: 18/09/03
Numerous medical studies have shown that exposure to blue light at night suppresses the production of melatonin by the pineal gland in our brains and so disrupts our circadian rhythms. As a result, we may have difficulty sleeping. It is therefore only common sense that we should specify warm white (3000 K) light sources wherever possible, especially for street lighting.
True or false?
To answer this question, we first need to define what we mean by “blue light.” Neither the Illuminating Engineering Society (IES) nor the Commission Internationale d’Eclairage (CIE) define the term in their online vocabularies. However, UL, LLC (formerly Underwriters Laboratories Inc.) has recently introduced its UL Verified Mark , a “third-party product claims verification program.” One such Verified Mark is shown in Figure 1:
The verification process for this mark is described thus:
“In accordance with LM-79-08, Section 9.1, measure the radiation emitted by the product across the visible spectrum of 380 – 780 nm. From the visible spectrum radiation measurement, determine the amount of ‘blue light’ radiation emitted between 440 – 490 nm. To calculate the percent of blue light emitted, divide the amount of blue light radiation by the amount of radiation measured across the complete visible spectrum.”
The lower wavelength limit of 440 nm seems somewhat arbitrary unless you also define “violet light,” but the upper wavelength limit of 490 nm makes sense; wavelengths in the region of 490 to 570 nm appear to be varying hues of green. This makes it easy – if we eliminate light of all wavelengths below 490 nm, we should not have any concerns about suppressing the production of melatonin and possible sleep disruption.
True or false?
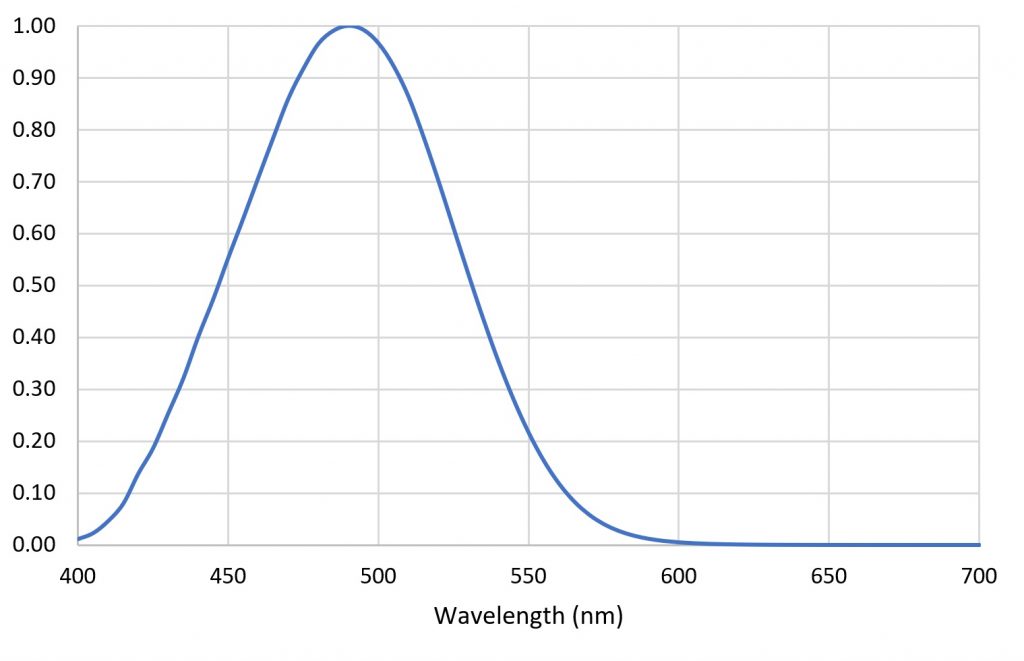
To answer this question, we need to take a closer look at those medical studies. The human retina has a smattering of intrinsically photosensitive retinal ganglion cells, or ipRGCs. Similar to the more familiar rods and cones, these ipRGCs contain a photosensitive protein called melanopsin. The sensitivity of melanopsin varies with wavelength, as shown in Figure 2.
It is these ipRGCs that sense “blue light” and send signals to the suprachiasmatic nucleus (SCN), a tiny region of some 20,000 neurons in the brain that is responsible for instructing the pineal gland when to produce melatonin.
Looking more closely at Figure 2, however, it is evident that the ipRGCs’ spectral sensitivity peaks at 490 nm, as well as extending to the ultraviolet edge of the visible spectrum at 380 nm. Most important, fully half the the spectral sensitivity of melanopsin is to green light.
Common sense is starting to look rather nervous …
The spectral sensitivity shown in Figure 2 is interesting enough, but it becomes even more so when we consider what it means for how we respond to the radiation emitted by white light LEDs.
Figure 3 shows the relative spectral power distributions (SPDs) of typical white light LEDs with correlated color temperatures (CCTs) of 3000 K and 4000 K, scaled such that both LEDs produce equal amounts of luminous flux.
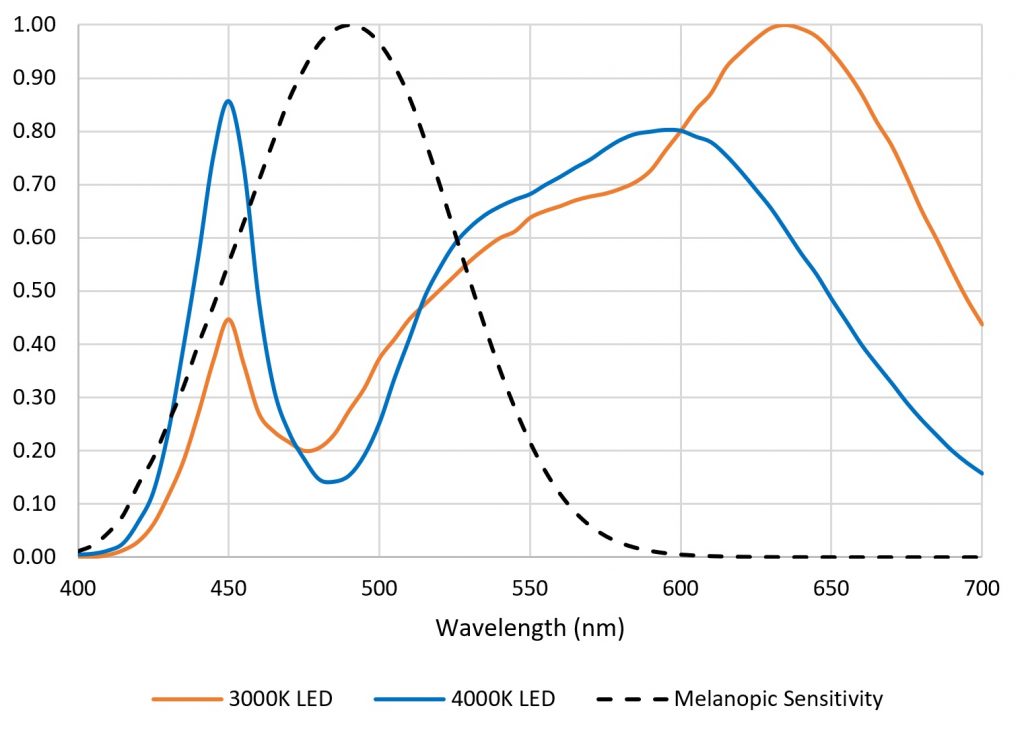
Determining the relative response of ipRGCs to these LEDS is easy – we simply multiply their SPDs by the melanopic sensitivity function on a per-wavelength basis, as shown in Figure 4.
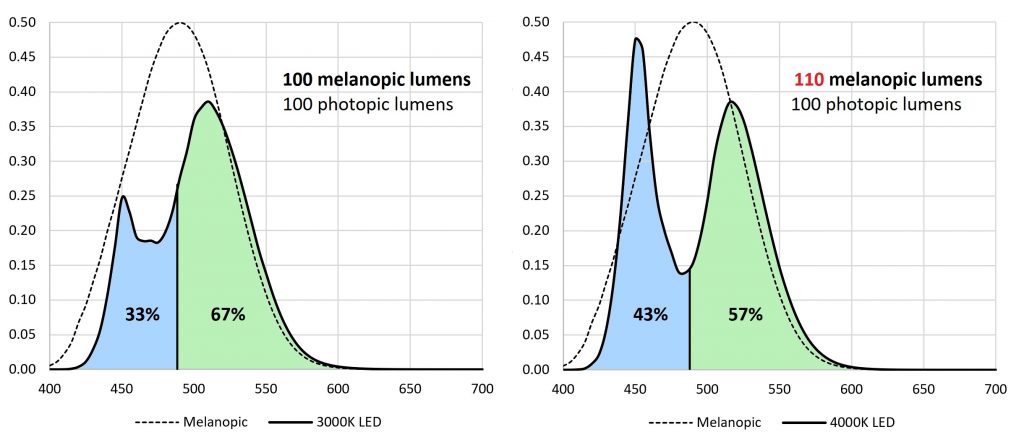
Common sense, it would seem, has good reason to be nervous. Yes, 3000-K LEDs produce less melanopic flux than 4000-K LEDs when they produce equal luminous flux. However, the difference is only ten percent. This is within the tolerance of architectural and roadway lighting design practices. As such, it should not be argued that 3000-K LEDs are required for nighttime lighting in order to minimize circadian rhythm disruption – the difference in melanopic flux does not support this. Rather, it is simply one of several factors that must be considered when designing and specifying lighting systems.
Blue-Blocking Glasses
Figure 4 highlights another issue: the efficacy of blue-blocking glasses, which are often marketed as promoting better sleep (Figure 5).

If we assume that the yellow filters provide a perfect cutoff at 490 nm, they are only 33% effective in blocking melanopic flux from 3000-K (warm white) LEDs and 43% effective with 4000-K (neutral white) LEDs. In reality, the filters likely let through some amount of blue light in the region of 470 nm to 490 nm, and so they may be even less effective.
Simply put, we cannot prevent melanopic flux emitted by white light sources from impacting our circadian rhythms unless we use deep-red filters. This is not to say that blue-blocking filters on eyeglasses or light sources do not work – they inarguably block blue light. However, melanopic flux includes both blue and green light.
From a marketing perspective, it is fair to say that blocking blue light may alleviate circadian rhythm disruption and loss-of-sleep issues, even if it is due to the placebo effect. (There are many other psychophysiological and environmental parameters involved in circadian rhythm entrainment that are not discussed here.) However, it is incorrect to claim that blocking blue light will eliminate melatonin suppression and so prevent circadian rhythm disruption. The facts state otherwise.
Electronic Devices
Finally, what about those evil electronic devices that threaten our sleep? Figure 6 shows the spectral power distribution of an Apple iPadÔ and the resultant melanopic flux when the display is set to full white (which has a CCT of 6700 K, somewhat higher than the 6500-K white point of most computer monitors).
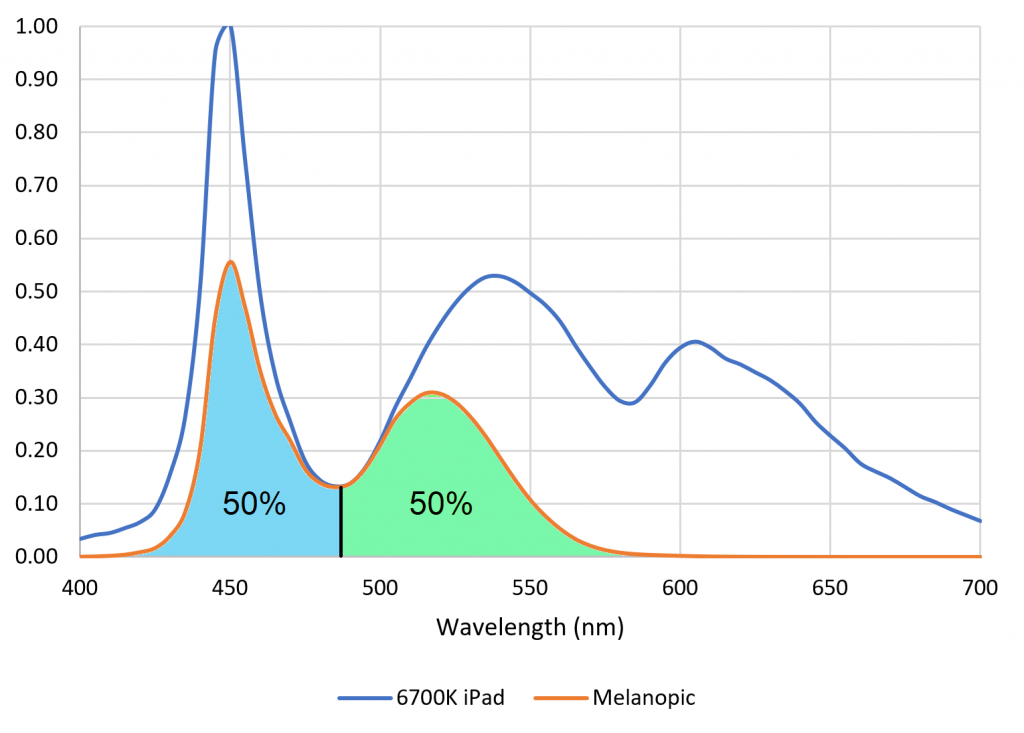
As shown by Figure 6, the best any optical filter or software-based change in the device white point (that is, a change in color temperature) can hope to achieve is a 50 percent reduction in melanopic flux.
What is more important, however, is that iPad screen luminance is approximately 400 cd/m2 (nits). This is on the order of 50 to 100 times the light levels recommended for residential street lighting. If we are to complain about light trespass from residential street lighting into our bedrooms causing sleep deprivation, we cannot ignore the influence of the televisions, computer monitors, and tablets that we often stare at for hours before going to bed, and in much closer proximity.
Conclusions
Research into the influence of spectral content and retinal illuminance on circadian rhythms is ongoing (e.g., Nagare et al., 2015). As such, this article should not be taken as evidence (or lack thereof) for the effect of “blue light” on our sleep patterns. Rather, it is a reminder to look beyond the marketing claims of “blue-light blocking” products and ask what this really means.
To answer the question of whether we should specify warm white (3000 K) light sources for street lighting, the answer is, “it depends.” All things being equal, the difference in melanopic flux between 3000-K and 4000-K LEDs is only ten percent. This is within the uncertainty of light design practices, and so more weight should be given to residents’ concerns, aesthetics, color discrimination, and energy savings when making design and specification decisions.
To answer the question of whether eliminating light of all wavelengths below 490 nm (that is, “blue light”) will eliminate any concerns about melatonin suppression and possible sleep disruption, the answer is clear: FALSE!
References
CIE. 2015. Report on the First International Workshop on Circadian and Neurophysiological Photometry, 2013. CIE Technical Note TN 003:2015.
Nagare, R., et al. 2017. “Does the iPad Night Shift Mode Reduce Melatonin Suppression?” Lighting Research and Technology.